Question 10#
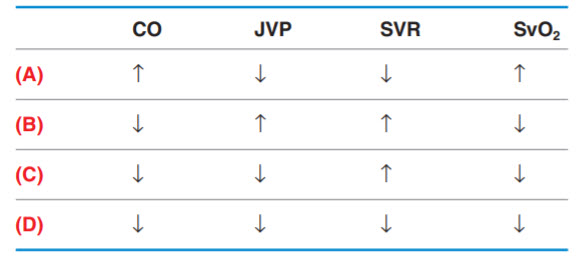
A 68-year-old man is brought in by ambulance after losing consciousness. The patient’s wife was with him when he developed crushing chest pain while lying in bed. His wife went to get him some medication for the pain, but when she returned the patient was unconscious. Paramedics were called, and an ECG showed ST elevations in the anterolateral leads. His blood pressure is extremely low, and his extremities are cool. Which of the following best represents the hemodynamics in this type of shock? (Note: CO is cardiac output, JVP is jugular venous pressure, SVR is systemic vascular resistance, and SvO2 is mixed venous oxygen saturation.)
A. (A)
B. (B)
C. (C)
D. (D)
Correct Answer is B
Comment:
Decreased CO, increased JVP, increased SVR, decreased SvO2. Cardiogenic shock can result from any process leading to ventricular failure, such as myocardial infarction, arrhythmias, acute valvular changes (e.g., acute mitral regurgitation), myocarditis, cardiac contusion, and exacerbated CHF. A decrease in cardiac output will manifest with distended neck veins and cool extremities since peripheral vessels will constrict (increased SVR) to preserve blood pressure. SvO2 indicates the oxygen saturation of hemoglobin in blood returning to the right side of the heart. In most causes of shock the SvO2 will be low due to poor circulatory function and increased tissue extraction of oxygen. SvO2 can be elevated in some forms of distributive shock (e.g., sepsis) due to a high flow state in which there is insufficient time for the peripheral tissues to extract oxygen from the circulating red blood cells. This patient suffered a myocardial infarction that led to cardiogenic shock.
Obstructive shock is a category in which the primary problem is not failure of the heart, but is an obstruction in the circulatory system that disrupts blood flow. Examples include pulmonary embolism, tension pneumothorax, and cardiac tamponade. This will present with the same hemodynamics given in the answer choice for cardiogenic shock; however, the two categories can be differentiated based on the history, physical examination, and other targeted studies.
(A) Examples of distributive shock include sepsis, anaphylaxis, adrenal insufficiency, and spinal cord injury (neurogenic shock). The primary problem in this form of shock is an inability to maintain SVR. The CO may be high initially but then will decrease over time due to cardiac fatigue. (C) In hypovolemic shock, SVR is increased as a response to maintain blood pressure but the CO is normal or low due to the decrease in preload. (D) This scenario could be seen in distributive forms of shock when the heart begins to fail, leading to a decrease in CO and subsequently SvO2 due to slowing of the previously high flow state.