Question 5#
An 82-year-old retired solicitor presents to the ED with chest pain radiating to his jaw. He has hypertension treated with ramipril 5 mg bd but is otherwise normally fit and well. His admission ECG shows atrial fibrillation with a ventricular rate of 90 bpm, LVH, and widespread ST segment depression. His peak troponin is 110 ng/L (normal <30 ng/L). He is started on treatment for an acute coronary syndrome and listed for an inpatient angiogram. You are asked to perform a bedside echocardiogram as a systolic murmur is heard on the post-take ward round.
His coronary angiogram shows:
- LMS: mild atheroma
- LAD: severe (90%) proximal stenosis; good distal target
- LCx: small vessel with diffuse distal atheroma
- RCA: dominant; moderate (50–60%) mid-vessel focal stenosis.
Which one of the following statements is correct?
A. The patient should be referred for AVR and LIMA to LADB. His operative mortality is about 3%
C. Surgical ablation for AF may be considered
D. The patient should have PCI to LAD followed by TAVI
E. He should be managed conservatively with a beta-blocker and warfarin
Correct Answer is C
Comment:
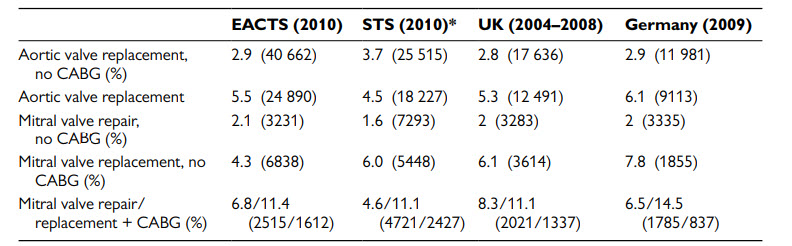
This patient has severe symptomatic aortic stenosis and two moderate to severe coronary stenoses with good distal targets. As he has no other significant comorbidity, he should be referred for AVR and two-vessel CABG. PCI and TAVI should be considered only if the patient is judged to be unsuitable for AVR after surgical consultation. In patients with a primary indication for aortic/mitral valve surgery, CABG is recommended for coronary artery stenosis ≥70% and should be considered for coronary artery stenosis ≥50–70% (ESC Guidelines 2012). This patient’s operative mortality for AVR and CABG is likely to be at least 4.5%. Table 3.2 shows the estimated operative mortality after surgery for valvular heart disease. AF is an independent risk factor for poor outcome after cardiac surgery. The ESC Guidelines for the management of AF recommend that surgical ablation should be considered in patients with symptomatic AF and may be performed in patients with asymptomatic AF undergoing cardiac surgery if feasible with minimal risk.
ESC guidelines 2012: operative mortality after surgery for valvular heart disease: