Question 17#
The following are true of hypercalciuria and its relation to stone formation, except:
A. It is often associated with calcium oxalate dihydrate stonesB. Can be treated with a thiazide diuretic
C. Is defined as the excretion of >5.5 mmol/24 hours of urinary calcium in a male
D. Can be associated with excessive salt intake
E. Can arise as a result of primary hyperparathyroidism
Correct Answer is C
Comment:
Answer C
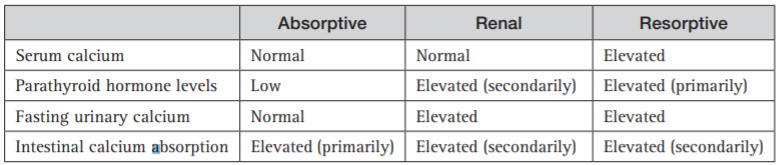
Hypercalciuria is defined as >4 mg/kg/24 hours or >7 mmol (men) or >6 mmol (women). Hypercalciuria can classified into idiopathic (50%), absorptive (from gut), renal leak or resorptive (from bone). In absorptive hypercalciuria, excessive calcium is absorbed from the gut leading to increased renal filtration and reduced renal reabsorption due to low parathyroid hormone and associated raised urinary phosphate (fasting urinary calcium is normal). Impaired tubular reabsorption of calcium (renal leak) occurs in 5%–10% of calcium stone formers and is characterised by fasting hypercalciuria with secondary hyperparathyroidism (raised PTH) but without hypercalcaemia. Resorptive hypercalciuria is almost always due to primary hyperparathyroidism which accounts for 3%–5% of all cases of hypercalciuria. The increased PTH levels leads to release of calcium from the bones as well as increasing calcium and vitamin D absorption from the bone and reducing calcium renal excretion from the distal tubule resulting in hypercalciuria (Table below). Excess salt intake can result in hypercalciuria, as sodium and calcium are co-transported in the kidney. Hypercalciuria is most commonly associated with calcium oxalate dihydrate stones.
Summary of the discriminating features of the different causes of hypercalciuria: