Question 4#
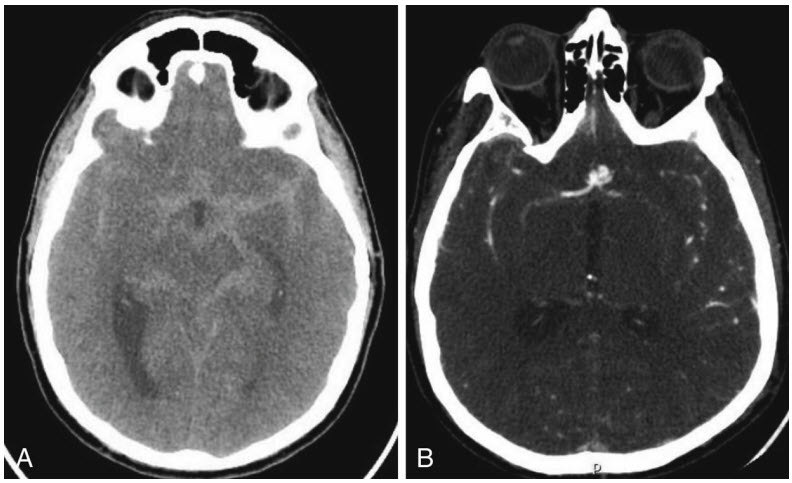
A 73-year-old woman with schizophrenia on lithium was found unresponsive by her husband in the bathroom. EMS was called, and on arrival she was unresponsive, intubated in the field, and brought to the ED. Her initial vital signs were stable and within normal limits. Off sedation, her eyes remained closed, minimally reactive pupils, no corneal or cough but intact gag reflex, and no movement to painful stimulation. A head CT, and CTA head and neck were completed (see figures below).
What is the patient’s Hunt and Hess and modified Fisher grade?
A. Hunt and Hess score 0 and Fisher grade 1B. Hunt and Hess score 5 and Fisher grade 4
C. Hunt and Hess score 5 and Fisher grade 3
D. Hunt and Hess score 0 and Fisher grade 4
Correct Answer is C
Comment:
Correct Answer: C
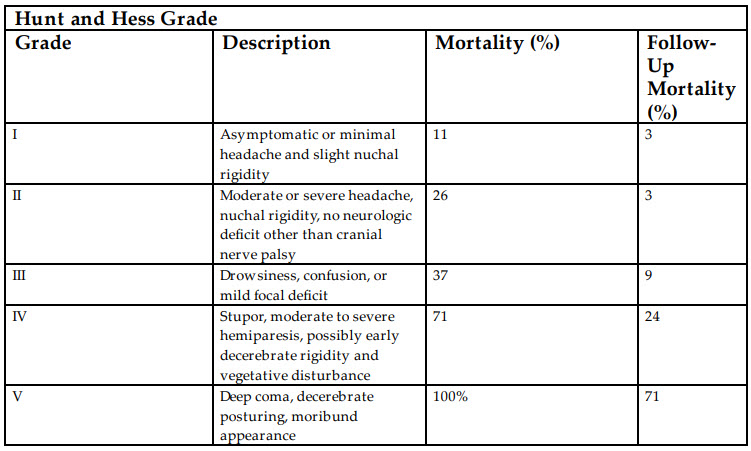
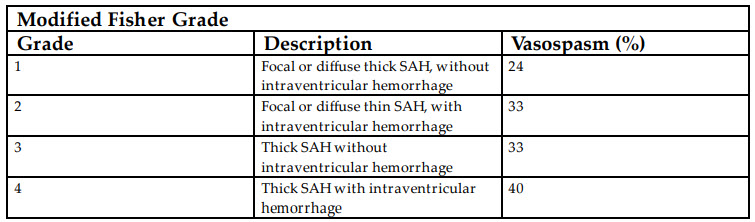
The patient presents with a subarachnoid hemorrhage in the setting of a basilar tip aneurysm which is seen on the sagittal reformatted images shown. The description of the patient’s presentation is best described by scales that have been previously developed that assist with long-term outcome as well as anticipated complications during the hospitalization. The Hunt and Hess score was developed as a tool for assessment of death. There are five grades with the lowest scores having better prognosis and higher having worse prognosis (Hunt and Hess Grade table). With the course of time and improved treatment strategies, the prognosis has improved, but those with the highest grade have a high mortality (71%). The Hunt and Hess grading system is based on the clinical exam of the patient. The second commonly used grading system for subarachnoid hemorrhage (SAH) is the modified Fisher scale (Modified Fisher Grade table). This is a radiographic-based scale which uses the thickness of subarachnoid blood and intraventricular extension to predict clinically relevant vasospasm. Vasospasm is a well-defined complication of subarachnoid hemorrhage which results in vasoconstriction of the cerebral vasculature through both calcium-dependent and calcium-independent pathways and results in cerebral ischemia.
References:
- Hunt WE, Hess RM. Surgical risks as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg. 1968;28:14-20.
- Antigua H, Ortega-Gutierrez S, Schmidt JM, et al. Subarachnoid hemorrhage: who dies, and why? Crit Care. 2015;31;309-316.
- Frontera JA, Claaassen J, Schmidt JM, et al. Prediction of symptomatic vasospasm after subarachnoid hemorrhage: the modified Fisher Scale. Neurosurgery. 2006;59:21-27.
- Kolas AG, Sen J, Belli A. Pathogenesis of cerebral vasospasm following aneurysmal subarachnoid hemorrhage: putative mechanisms and novel approaches. J Neurosci. 2009;87:1-11.