Question 3#
A 68-year-old male with a past medical history of hypertension arrives at the Emergency Department with crushing chest pain. The pain started 1 hour ago and is substernal with radiation to his left shoulder. He is mildly diaphoretic and dyspneic. Vital signs on presentation are notable for:
- a blood pressure of 110/65 mm Hg
- heart rate of 100 beats per minute
- oxygen saturation of 99% on room air
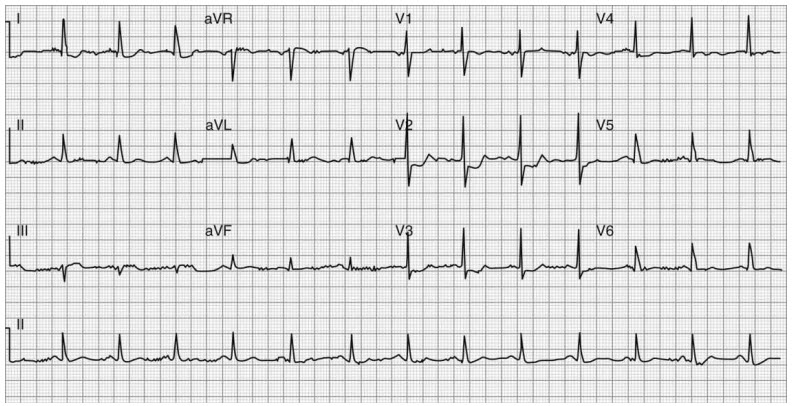
His initial ECG is shown in the figure below:
Which of the following is the next BEST step to evaluate the extent of cardiac damage in this patient?
A. TroponinB. CK-MB
C. Right-sided ECG leads
D. Posterior ECG leads
E. Right-sided heart catheterization
Correct Answer is D
Comment:
Correct Answer: D
This patient has ST segment depressions in the anteroseptal leads (V2- V4), and early R wave progression. The ST segment changes may be interpreted as anterior ischemia in the context of a non-ST segment elevation myocardial infarction, posterior STEMI is an important differential. The early R wave progression here indicates the evolution of Q waves in the posterior wall of the heart. Posterior MI accompanies ∼15%-20% of STEMIs, most commonly inferior or lateral STEMI due to perfusion of these territories and the posterior territory usually by the right coronary artery. The next most important test that can be done at bedside is to better characterize this is posterior ECG leads (V7-V9). The posterior MI leads are located in the same horizontal plane as V6, located at the posterior axillary line (V7) and paraspinal (V9), with V8 in between. If posterior leads confirm ST segment elevation, noting that the AHA/ACC guideline requires only 0.5 mm of ST segment elevation in these posterior leads, then the patient should be triaged for emergent coronary angiography.
Ultimately troponins and CK-MB are important in characterizing myocardial damage and impacting treatment and prognostication, but the first step should be to exclude a STEMI in a patient with this pattern on ECG. A right-sided ECG would be important in a patient presenting with an inferior MI to evaluate for RV infarction.
References:
- van Gorselen EO, Verheugt FW, Meursing BT, Oude Ophius AJ.Posterior myocardial infarction: the dark side of the moon. Neth Heart J. 2007;15(1):16-21.
- Thygesen K, Alpert JS, Jaffe AS, et al; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618-e651. doi:10.1161/CIR.0000000000000617.