Question 2#
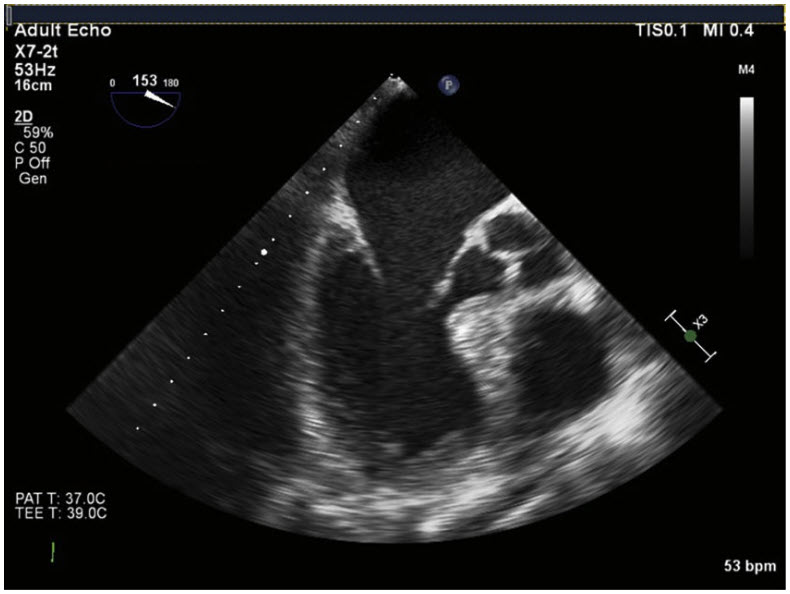
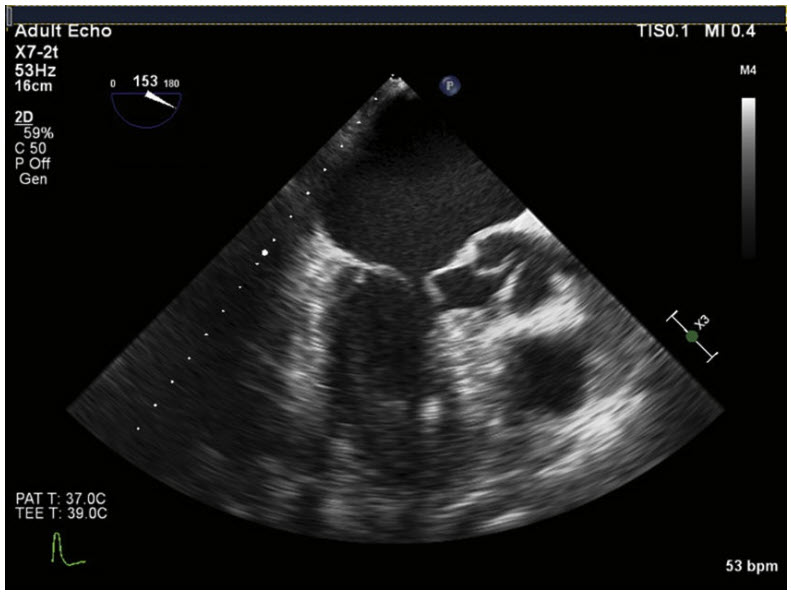
A 55-year-old man underwent bilateral lung transplantation for idiopathic pulmonary fibrosis with intraoperative central venoarterial ECMO support. After implantation of the second lung, the team is unable to wean the patient off the ECMO circuit despite dobutamine and norepinephrine infusions. TEE images of the midesophageal long axis view at end-diastole (A) and mid-systole (B) are shown in the figures below.
Based on the TEE findings, which of the following is the next best step in management?
A. Add epinephrine infusionB. Insert an intra-aortic balloon pump
C. Discontinue dobutamine
D. Perform aortic valve replacement
Correct Answer is C
Comment:
Correct Answer: C
The diastolic picture shows a mid-esophageal long axis view of the left atrium, left ventricle, mitral valve, and aortic valve. The basal septum appears disproportionately thick, but without more information one cannot distinguish between disproportionate upper septal thickening and hypertrophic cardiomyopathy (HCM). In the systolic frame, one can see several abnormalities. The anterior leaflet of the mitral valve has moved into the left ventricular outflow tract (LVOT). A visible space is seen between the anterior and posterior mitral leaflets, which should have a tight coaptation point in systole. The aortic valve, which should be widely open during systole, appears only partially open. Taken together these findings lead to the diagnosis of systolic anterior motion (SAM) of the mitral valve. In SAM, the mitral valve moves into the LVOT during systole, creating an outflow tract obstruction. The force of the blood moving through the LVOT may pull the anterior mitral leaflet away from the posterior leaflet, leading to mitral regurgitation. The interrupted systolic ejection can lead to early aortic valve closure or partial opening in systole. SAM is most commonly seen in HCM or after mitral valve repair. However, it can also be seen in hyperdynamic or hypovolemic states, when small LV size combined with excessive inotropy can lead to SAM in otherwise normal hearts.
Medical management of SAM hinges around volume loading, reducing inotropy, and increasing peripheral resistance. Therefore, stopping the dobutamine infusion would be the first step of the options provided. Adding epinephrine would likely worsen the SAM through increased inotropy and reduced diastolic filling time. An intra-aortic balloon pump reduces LV afterload and would not be beneficial here. Finally, the aortic valve likely has no pathology and only opens incompletely due to a small stroke volume (SV). Valve replacement is not indicated.
Reference:
- Ibrahim M, Rao C, Ashrafian H, Chaudhry U, Darzi A, Athanasiou T. Modern management of systolic anterior motion of the mitral valve. Eur J Cardiothorac Surg. 2012;41(6):1260-1270.