Question 4#
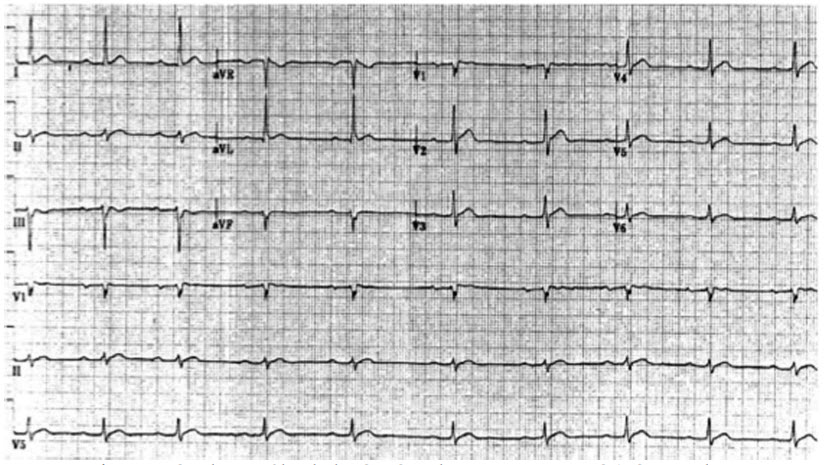
A 47-year-old male with a PMH of lung cancer presents with confusion and lethargy. He has postural hypotension and low central venous pressure on examination. There is no fever, cough, sputum, or rash. The remainder of the examination is notable only for tachycardia. CXR shows a right upper lobe mass similar to prior films and mediastinal lymphadenopathy and left lower lobe nodules. Serum creatinine is 2 mg/dL. Serum calcium is 18 mg/dL and electrocardiogram EKG is shown in the figure below:
What is the most appropriate treatment?
A. Measurement of serum albuminB. Saline and furosemide
C. Pamidronate
D. Head CT
Correct Answer is B
Comment:
Correct Answer: B
This patient with advanced lung cancer (lymphadenopathy and contralateral nodules on CXR, in addition to the presumably primary lung mass) is presenting with severe hypercalcemia, which is a medical emergency. Hypercalcemia of malignancy is a late complication in a number of tumors and is associated with poor outcomes. Up to one-half of all patients diagnosed with malignancy-associated hypercalcemia will die within a month of diagnosis. Serum calcium levels are regulated by a balance between bone resorption, intestinal absorption, and renal excretion. Parathyroid hormone (PTH) modulates all of these processes by increasing bone resorption, decreasing renal calcium excretion, and increasing intestinal excretion by converting calcidiol to calcitriol. Hypercalcemia can occur in malignancy via direct osteolysis in the case of bony metastasis, ectopic PTH secretion, or the action of PTH-related proteins. Therapy for hypercalcemia includes aggressive volume repletion, loop diuretics to maintain high urine output, and bisphosphonates such as pamidronate to decrease bone resorption. While pamidronate should be initiated as soon as hypercalcemia is diagnosed, the peak effect is not achieved for 2 to 4 days making other supportive measures, such as fluid resuscitation, important. Serum calcium measurements can be affected by albumin, and there exist formulas for the correction of measured calcium for hypoalbuminemia. However, this patient has classic signs of hypercalcemia (including shortened QT interval of EKG, altered mental status, and hypovolemia) as well as very elevated uncorrected calcium. Head CT is an important part of the workup of altered mental status, but there is adequate evidence to support a diagnosis of hypercalcemia, and treatment should be initiated as soon as possible.
References:
- McCurdy MT, Shanholtz CB. Oncologic emergencies. Crit Care Med. 2012;40:2212-2222.
- Stewart AF. Hypercalcemia associated with cancer. N Engl J Med. 2005;352:373-379.