Question 5#
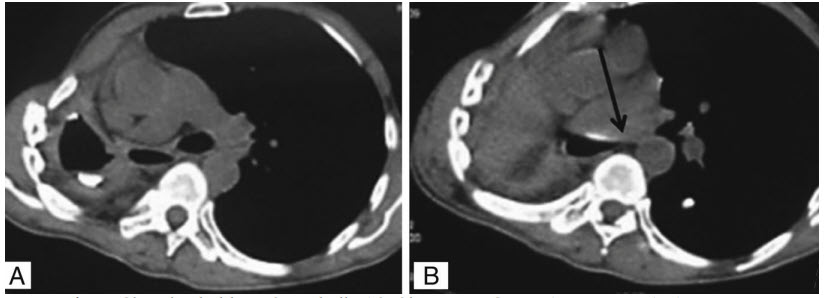
A 60-year-old female was diagnosed with right-sided proximal bronchogenic carcinoma and underwent right-sided pneumonectomy 8 months ago. She presents to the ED with a 1- month history of progressive dyspnea, cough, stridor, and occasional low-grade fevers. A CT chest was performed and shown in the two figures below:
What should be the next step in management?
A. Insertion of a chest tubeB. Barium swallow study
C. IV steroids
D. Surgery
Correct Answer is D
Comment:
Correct Answer: D
The image demonstrates stretching of the left main bronchus between the pulmonary artery and vertebral body which can occur in postpneumonectomy syndrome. Postpneumonectomy syndrome is a rare complication that typically occurs 6 months or later after pneumonectomy. It is characterized by extreme shift of the mediastinum, and common symptoms include increasing dyspnea, cough, stridor, and recurrent pulmonary infections. The syndrome is more common after right-sided pneumonectomy as there is greater volume loss with removal of the right lung. Treatment for postpneumonectomy syndrome involves shifting the mediastinum closer to the midline to remove the compression on the airway and vessels. This procedure is typically performed by inserting saline-filled prostheses on the side of the pneumonectomy. A chest tube would be an appropriate next step for empyema formation, which can be a late complication of pneumonectomy. On imaging, this could be characterized by air fluid levels or a loculated pleural effusion on the side of the surgery which was not visualized in this patient. A barium swallow would be helpful in diagnosing an esophagopleural fistula. An esophagopleural fistula in the late stages is typically caused by residual tumor burden eroding into the esophagus. It will typically present with an empyema, and a barium swallow will demonstrate the spilling of contrast into the airway. Finally IV steroids can be used for pulmonary edema that can occur post pneumonectomy. This is typically an early complication within 72 hours of surgery, therefore would not fit with this patient’s delayed time course.
References:
- Chandrashekhara SH, Bhalla AS, Sharma R, Gupta AK, Kumar A, Arora R. Imaging in postpneumonectomy complications: a pictorial review. J Cancer Res Ther. 2011;7(1):3-10. PubMed PMID:21546734.
- Sharifpour M, Bittner EA. Postpneumonectomy syndrome: a case of shifting priorities. Anesthesiology. 2014;121(6):1334. PubMed PMID:24047857.