Question 7#
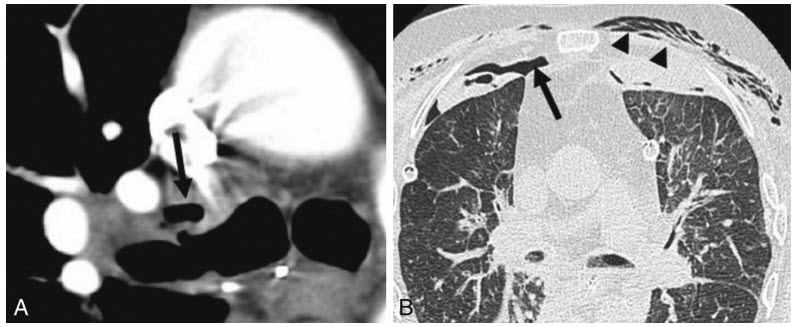
A 52-year-old man with severe COPD underwent bilateral lung transplant 10 days ago. His postoperative course was unremarkable. He was extubated and transferred to the floor on postoperative day 5. Today, he starts to complain of shortness of breath. The physical examination is significant for chest wall subcutaneous emphysema. Images from a chest CT scan below:
What is the BEST next step in management?
A. Pulse dose of methylprednisoloneB. Flexible bronchoscopy
C. Open surgical exploration and repair
D. Observation and serial chest x-rays
Correct Answer is B
Comment:
Correct Answer: B
Bronchial dehiscence is a feared complication after lung transplantation. Its incidence ranges between 1% and 10% of all lung transplantation. Bronchial arterial circulation is usually not reconstructed during transplant which could lead to bronchial ischemia and dehiscence. Bronchial artery circulation typically reestablished within 4 weeks by collateral formation. Bronchial dehiscence is classified as a partial or complete, and it usually occurs within the first 5 weeks postoperatively. Patients typically present with dyspnea, pneumomediastinum, pneumothorax, persistent chest tube air leak, or subcutaneous emphysema.
Chest CT is highly sensitive and specific for diagnosing bronchial dehiscence. Radiological signs such as bronchial wall defects, bronchial wall irregularities, or extraluminal air around anastomosis area are suggestive for bronchial dehiscence. Although CT scan is an excellent diagnostic modality, flexible bronchoscopy remains essential for making the final diagnosis. CT scan is not reliable for detecting mucosal necrosis as bronchoscopy. Moreover, bronchoscopy is superior to CT scan in assessing the severity of dehiscence. Depending on the severity of bronchial dehiscence, management could include conservative treatment, bronchoscopic or open repair. Conservative treatment includes antibiotics and close monitoring. Bronchoscopic interventions include the use of stents, cyanoacrylate glue, growth factors, and autologous platelet-derived wound-healing factor. Open repair includes reanastomosis, flap bronchoplasty, pneumonectomy, or retransplantation.
Acute rejection (answer A) is in the differential diagnosis for any posttransplant lung transplant patients with shortness of breath; however, CT scan results and physical examination in this patient suggest airway complication rather than rejection. Confirmation of diagnosis and severity assessment should be done by flexible bronchoscopy to guide management (answer B). Serial chest x-ray has no role in confirming or evaluation of the severity of bronchial dehiscence (answer D).
References:
- Habre C, Soccal PM, Triponez F, et al. Radiological findings of complications after lung transplantation. Insights Imaging. 2018. doi:10.1007/s13244-018-0647-9.
- Santacruz JF, Mehta AC. Airway complications and management after lung transplantation: ischemia, dehiscence, and stenosis. Proc Am Thorac Soc. 2009;6(1):79-93. doi:10.1513/pats.200808-094GO.
- Mahajan AK, Folch E, Khandhar SJ, et al. The diagnosis and management of airway complications following lung transplantation. Chest. 2017;152:627-638.