Question 8#
A 38-year-old male is brought to the hospital after a witnessed seizure. The patient’s medical history is only significant for bipolar disease. His sister also reports that he recently started a new diet regimen using herbal supplements that he purchased online. On physical examination, his vital signs are unremarkable. He appears unkempt, and there is a small laceration noted over his tongue. His serum sodium is 128 mEq/L (mmol/L). Other laboratory findings before and after water deprivation test (WDT) are shown below:
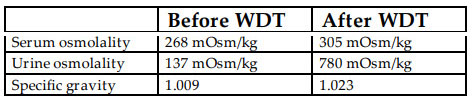
What is the MOST likely diagnosis in this patient?
A. Nephrogenic DIB. Pseudohyponatremia
C. Psychogenic polydipsia
D. SIADH
E. Central DI
Correct Answer is C
Comment:
Correct Answer: C
The cause for his hyponatremia is due to increased free water intake which may manifest in patients with underlying psychiatric disorders, such as schizophrenia, depression, and bipolar disorder in particular. When patients present with polyuria, WDT can help differentiate between psychogenic polydipsia and DI. It is believed that patients with psychogenic polydipsia have a dysregulated thirst mechanism with a reduced osmotic threshold for thirst compared to the ADH threshold, causing them to drink more than needed. It rarely occurs as the amount of free water intake needed to cause hyponatremia is greater than 7 L/d. In patients with polydipsia, an increase in serum osmolarity from water deprivation leads to a marked increase in urine osmolality. On the other hand, urine osmolality will remain low in a patient with DI. Other important differentiating feature is that DI causes hypernatremia while patients with polydipsia are either eunatremic or mildly hyponatremic. Desmopressin has no effect since endogenous release is intact. SIADH and pseudohyponatremia do not cause polyuria.
References
- Goldman MB. The influence of polydipsia on water excretion in hyponatremic, polydipsic, schizophrenic patients. Endocrinol Metab. 1996;81(4):1465-1470.
- Hariprasad MK, Eisinger RP, Nadler IM. Hyponatremia in psychogenic polydipsia. Arch Intern Med. 1980;140(12):1639-1642.
- Trimpou P, Olsson DS, Ehn O, Ragnarsson O. Diagnostic value of the water deprivation test in the polyuria-polydipsia syndrome. Hormones (Athens). 2017;16(4):414-422.