Question 1#
A 78-year-old lady was found at her home after a fall earlier in the day by her daughter. Medication history is significant for aspirin, statin, glipizide, and acetaminophen use for chronic low back pain. She recently visited her primary care physician with significant weight loss and failure to thrive. She is currently admitted in the intensive care unit (ICU) for multiple rib fractures and flail chest. Her urine analysis and labs are as follows:
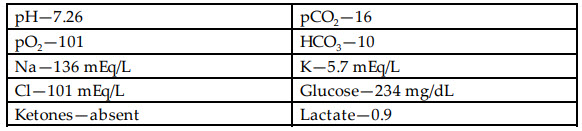
What is the most likely cause for her acid-base abnormality and hyperkalemia?
A. Ketones from starvation ketosisB. 5-Oxoproline
C. Isopropyl alcohol
D. Lactic acidosis
Correct Answer is B
Comment:
Correct Answer: B
This patient has high anion gap metabolic acidosis with resultant acidosis-induced hyperkalemia. One of the overlooked causes of metabolic acidosis is elevation of serum oxoproline levels, seen more commonly in undernourished patients taking acetaminophen regularly. The patient has no lactate or ketones in their lab workup. Isopropyl alcohol toxicity causes an osmolar gap only and no anion gap (choices A, C, and D are incorrect). Causes of high anion gap metabolic acidosis can be remembered with the mnemonic—GOLDMARK:
- Glycols
- Oxoproline
- L-Lactate
- D-Lactate
- Methanol
- Aspirin
- Renal failure
- Ketoacidosis
When a source of high anion gap metabolic acidosis is not obvious, elevated 5-oxoproline level (also called pyroglutamic acid) should be considered, especially if there is a history of acetaminophen use.
References:
- Mehta A, Emmett JB, Emmett M. GOLD MARK: an anion gap mnemonic for the 21st century. Lancet. 2008;372(9642):892.
- Aronson PS, Giebisch G. Effects of pH on potassium: new explanations for old observations. J Am Soc Nephrol. 2011; 22:1981.