Question 3#
A 59-year-old female with a history of hypertension and gout is admitted in the ICU for observation status post thrombolysis for ischemic stroke. Her outpatient medications include metoprolol, colchicine, aspirin, metformin, and meloxicam. Vitals are normal except for sinus tachycardia with a heart rate (HR) of 108 beats per minute. Low bicarbonate is noted on labs prompting an arterial blood gas (ABG), and patient is found to be mildly acidotic. Lab values are given below:

Urine electrolytes:
- Na—56 mEq/L
- K—10 mEq/L
- Cl—56 mEq/L
Which of the following can most likely be expected to be the cause of this?
A. Chronic diarrheaB. Type 1 renal tubular acidosis
C. Type 4 renal tubular acidosis
D. Bartter syndrome
Correct Answer is C
Comment:
Correct Answer: C
The blood gas suggests a metabolic acidosis. The anion gap is 12, which is appropriate for an albumin of 4. There is no respiratory-driven acidosis component as denoted by normal pCO2 of 38 mm Hg. This patient has NAGMA. The next step is to calculate the UAG
U.Na + U.K - U.Cl = 56 + 10 - 56 = 10
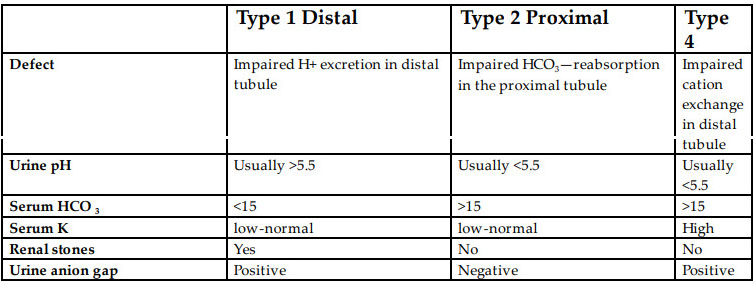
A positive numerical value on UAG in NAGMA can be seen in renal tubular acidosis (type 1 and type 4), spironolactone, and acetazolamide use. This patient has serum chemistry consistent with renal tubular acidosis type 4 with hyperkalemia not explained by any other etiology. Types of renal tubular acidosis with their respective differentiating features are depicted in the table below:
References:
- Goldstein MB, Bear R, Richardson RMA, Marsden PA, Marsden ML, Haleperin ML. The urine anion gap: a clinically useful index of ammonium excretion. Am J Med Sci. 1986;292(4):198-202.
- Soriano JG. Renal tubular acidosis: the clinical entity. J Am Soc Nephrol. 2002;13:2160-2170.