Question 6#
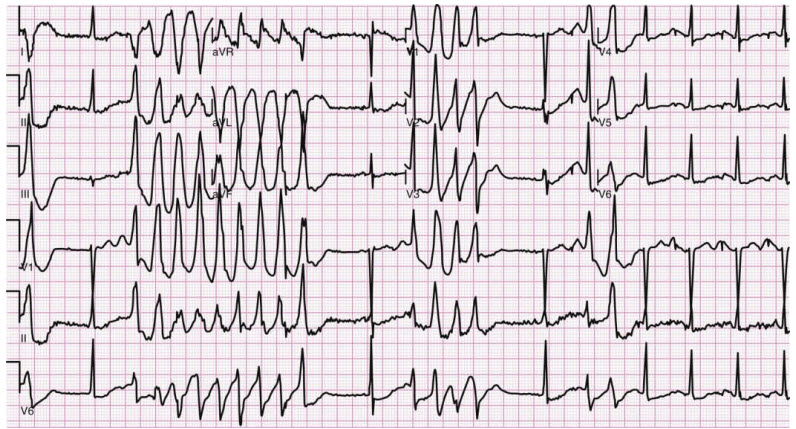
A 54-year-old male presents to the emergency department with agitation. The ED physician orders haloperidol for agitation before learning that patient is taking high-dose methadone for back pain and has a history of substance abuse and dependence. Labs are awaited. His ECG strip on telemetry is shown in the figure that follows. He converts to normal sinus rhythm after receiving 2 g of magnesium. 10 minutes later the arrhythmia shown below recurs. He is alert and talking comfortably Vitals:
- BP: 110/68
- SpO2 : 94% on 2 L/min oxygen via nasal cannula
What should be the next immediate step?
A. Give more magnesiumB. Synchronized cardioversion
C. IV isoproterenol to increase heart rate
D. Overdrive pacing to increase heart rate
Correct Answer is A
Comment:
Correct Answer: A
The management of Torsades de Pointes begins with assessing if the patient is hemodynamically stable. Most episodes of torsades are selflimiting. However, the danger lies in those patients who go on to develop ventricular fibrillation. Synchronized cardioversion should be performed on a hemodynamically unstable patient in torsades who has a pulse (100 J monophasic, 50 J Biphasic). Pulseless torsades should be defibrillated.
This patient is hemodynamically stable. Studies have shown that levels of magnesium drop precipitously a short time after a bolus infusion. It is recommended to start an infusion soon after the bolus dose of magnesium or supplement with intermittent magnesium pushes and follow labs for magnesium levels and monitor patient for magnesium overdose effects.
References:
- Biesenbach P, Mårtensson J, Lucchetta L, et al. Pharmacokinetics of magnesium bolus therapy in cardiothoracic surgery. J Cardiothorac Vasc Anesth. 2018;32(3):1289-1294.
- Tzivoni D, Banai S, Schuger C, et al. Treatment of torsade de pointes with magnesium sulfate. Circulation. 1988;77(2):392-397.