Question 5#
A 64-year-old woman is being treated in the local intensive care unit (ICU) for septic shock due to Streptococcus pneumoniae. She weighs 120 kg. She is started on empiric antibiotics and resuscitated with 30 mL/kg of normal saline without significant improvement. She is therefore temporarily started on vasopressor support. She improves after 4 days and is weaned off all vasopressors. She extubated to noninvasive ventilation. However, her voice remains hoarse, and she fails her swallow evaluation. She remains on intravenous fluids for hydration for 3-day history of diarrhea.
Laboratory data obtained on admission:
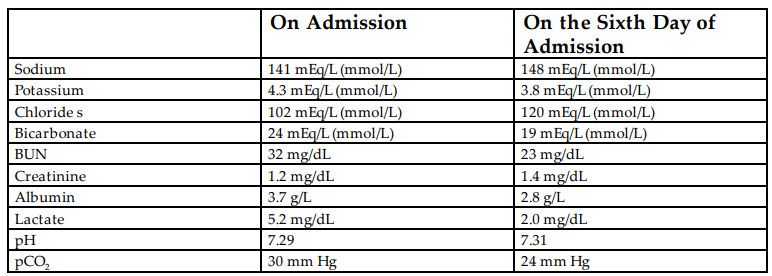
What is the MOST likely cause for her laboratory abnormalities?
A. Contraction alkalosisB. Diuresis
C. Fluid administration
D. RTA
E. Hypoalbuminemia
Correct Answer is C
Comment:
Correct Answer: C
Iatrogenic causes of non–anion gap metabolic acidosis are common in the setting of critical ill patients, who require aggressive fluid administration, particularly when chloride-rich solutions such as 0.9% saline are used. When large amounts of sodium chloride–containing solutions are administered, the chloride concentration in the serum will rise more than that of sodium as the serum chloride levels are normally lower than serum sodium. Therefore, the strong ion difference (SID) decreases and leads to a reduction of the positive plasma charge. To compensate for this, the chloride reacts with bicarbonate to produce protons and buffer the pH. This leads to depletion of bicarbonate stores and subsequently an acidosis.
Reference:
- Kraut J, Kurtz I. Treatment of acute non-anion gap metabolic acidosis. Clin Kidney J. 2015;8(1):93-99.