Question 4#
A 63-year-old man is admitted to the ICU after exploratory laparotomy, superior mesenteric artery (SMA) thrombectomy, and small bowel resection. He received 2 L of crystalloid resuscitation in the operation room, and his estimated blood loss was 150 mL. He did not receive transfusion in the operating room. His:
- white blood count is 20,000 cells/microL with 90% neutrophils
- hemoglobin 19.1 g/dL
- hematocrit 57%
- platelet count 265,000 platelets/microL
Which of the following statements regarding his laboratory data is MOST correct?
A. His complete blood count (CBC) likely reflects a volume depleted state and no further workup is necessaryB. He cannot have polycythemia vera (PV) if the JAK2V617F mutation is not detected
C. If he has PV, he should be treated with aspirin alone
D. His serum EPO level should be low if he has PV
Correct Answer is D
Comment:
Correct Answer: D
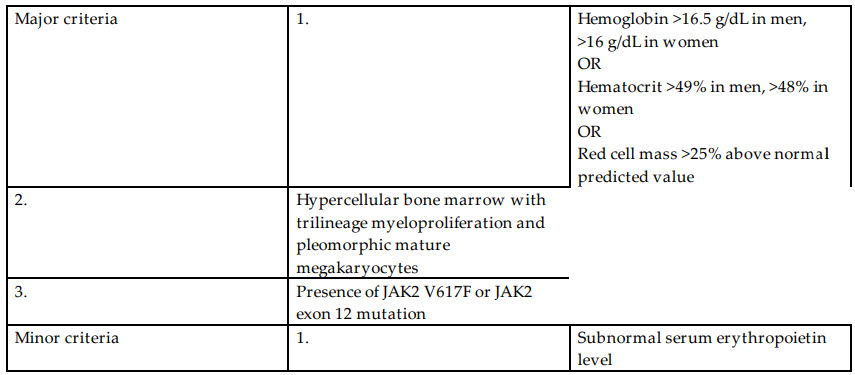
Although the differential diagnosis of an elevated RBC mass is large including volume contraction, chronic hypoxia, and exogenous EPO, PV should be suspected in a patient with unusual thrombosis, thrombocytosis and/or leukocytosis, or splenomegaly. PV is a chronic myeloproliferative neoplasm characterized by an increased RBC mass. It is associated with an increased risk of thrombosis (both arterial and venous), leukemic transformation, and myelofibrosis. Workup for PV should include EPO level and peripheral blood mutation screening for JAK2 V617F. The World Health Organization diagnostic criteria for PV are listed in Table below. Either all three major criteria or the first two major criteria plus the minor criterion is needed for the diagnosis of PV.
The presence of the JAK2 V617F mutation is 97% sensitive and 100% specific for PV. The addition of a low EPO level confirms the diagnosis. Additional mutational analysis for the JAK2 exon 12 mutation should be pursued if the EPO level is low and the JAK2 V617F mutation is not present as 3% of patients with PV are JAK2 V617F-negative.
All patients with PV require phlebotomy to a hematocrit target of <45%. Other treatment depends on risk stratification based on age, history of prior thrombosis, and cardiovascular risk factors. Patients younger than 60 years of age without history of thrombosis can be treated with observation alone or aspirin depending on cardiovascular risk factors. Patients older than 60 years of age or with a history of thrombosis should be treated with aspirin and a cytoreductive agent. Hydroxyurea, interferon alfa, and busulfan are all acceptable initial therapies for PV.
2016 World Health Organization Diagnostic Criteria for Polycythemia Vera:
References:
- Khan FA, Khan RA, Iqbai M, et al. Polycythemia vera: essential management protocols. Anaesth Pain Intensive Care. 2012;16: 91-97.
- Tefferi A, Barbul T. Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management. Am J Hematol. 2017;92:95-108.
- Tefferi A, Vannucchi A, Barbui T. Polycythemia vera treatment algorithm 2018. Blood Cancer J. 2018;8:3.