Question 1#
A 30-year-old man complains of unilateral headaches. He was diagnosed with migraine headaches at age 24. The headaches did not respond to triptan therapy at that time, but after 6 weeks the headaches resolved. He has had three or four spells of severe headaches since then. Currently his headaches have been present for the past 2 weeks. The headaches start with a stabbing pain just below the right eye. Usually the affected eye feels “irritated” (reddened with increased lacrimation). He saw an optometrist during one of the episodes and a miotic pupil was noted. Each pain lasts from 60 to 90 minutes, but he may have several discrete episodes each day. The neurological examination, including cranial nerve examination, is now normal.
What is your best approach to treatment at this time?
A. Prescribe oral sumatriptan for use at the onset of headacheB. Prednisone 60 mg daily for 2 to 4 weeks
C. Obtain MRI scan of the head with gadolinium contrast
D. Begin propranolol 20 mg bid
E. Refer for neuropsychiatric testing
Correct Answer is B
Comment:
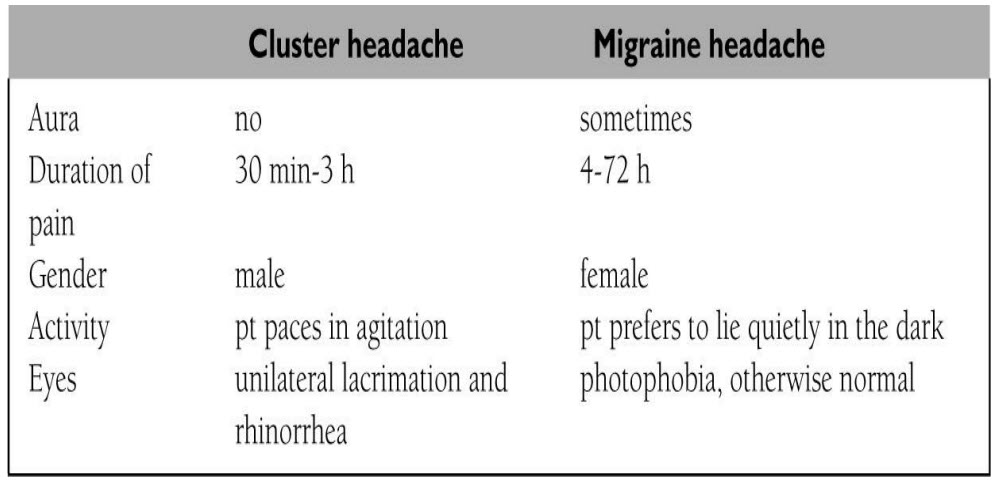
The history is classic for cluster headache, an often debilitating periodic pain syndrome. The typical cluster lasts for weeks and then remits. Like classic migraines, cluster headaches are unilateral and can be associated with autonomic symptoms (including Horner syndrome) on the symptomatic side. The following chart helps you to distinguish cluster headache from migraine:
Treatment of cluster headache involves two principles: (1) aborting the cluster and (2) relieving the headache when it occurs. Prednisone is usually given to abort the cluster; 40 to 60 mg per day is given for weeks and then tapered over a month or two. Propranolol and tricyclic antidepressants (which are given for migraine prevention) are much less helpful in the patient with cluster headache. Verapamil and carbamazepine are sometimes used if prednisone is ineffective. It is harder to relieve the individual headache in cluster disorder because each episode of pain is of shorter duration than in migraine. Triptans or high-flow oxygen (7-10 L per minute via face mask) may be effective. The pain in cluster headache is very severe, and suicides have occurred when the patient enters another stereotypical cluster. Proper diagnosis and treatment are therefore crucial. Neuroimaging studies are not indicated unless atypical features or focal neurological findings are present. Neuropsychiatric testing is expensive and would not be indicated in this patient with classic cluster headache.